

Alex Loh BDSc(Hons) GradDipClinDent(Impl) GradDipClinDent(Orth) FRACDS FICCDE FIADFE
Dr Alex Loh is a dedicated dentist who has been involved in implant restoration since 2008, at a time when direct-to-fixture restorations were not commonly practiced. His interest in implantology led him to achieve Fellowship status with the Royal Australasian College of Dental Surgeons in 2012, specialising in Restorative and Periodontics. Driven by a passion for continued learning, he attended prestigious continuing education courses and completed a Graduate Diploma in Clinical Dentistry (Dental Implantology) in 2017. He is also a Fellow of the International College of Continuing Dental Education and the International Academy of Dental Facial Esthetics.
Dr Loh’s pursuit of knowledge extends to orthodontics as well. He obtained a Graduate Diploma in Clinical Dentistry (Orthodontics) and is currently working towards a Master’s degree in Clinical Dentistry (Orthodontics) at The University of Bolton.
Throughout his career, Dr Loh has observed the changing paradigms in implant restoration. However, he has also noticed a lack of educational programs focused on the restorative aspects of implantology, despite technical complications being more prevalent than biologic complications according to systematic reviews of the literature. Driven by a commitment to bridge this educational gap, he provides comprehensive training to general dentists in these critical areas of dentistry.
Introduction
The use of cement-retained or screw-retained implant prostheses has long been debated in the literature. Articles have been published from more than 20 years ago1 till very recently2 discussing the advantages and disadvantages of either approach.
Despite the numerous articles published, many fail to clearly define the terms screw-retained or cement-retained. The exact definition of either of these terms is missing from the articles3,4,5,6,7,8,9,10, or at best, is vague1.
The aim of the first of this three part article is to clarify the meaning of these terms used in the literature, and then use this knowledge in the final part of this article to describe the solution to a clinical case involving a patient’s restorative complication when implant components are used incorrectly. The second part will discuss the concept of abutment indexing, when they are required, and how it relates to the solutions of the clinical case report.
Lack of Definition Clarity for Cement-Retained and Screw-Retained Prostheses
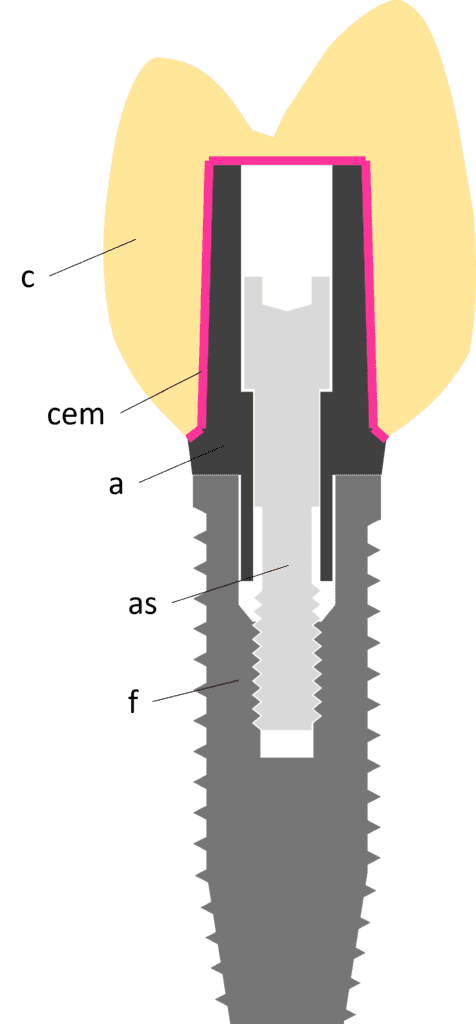
Figure 1
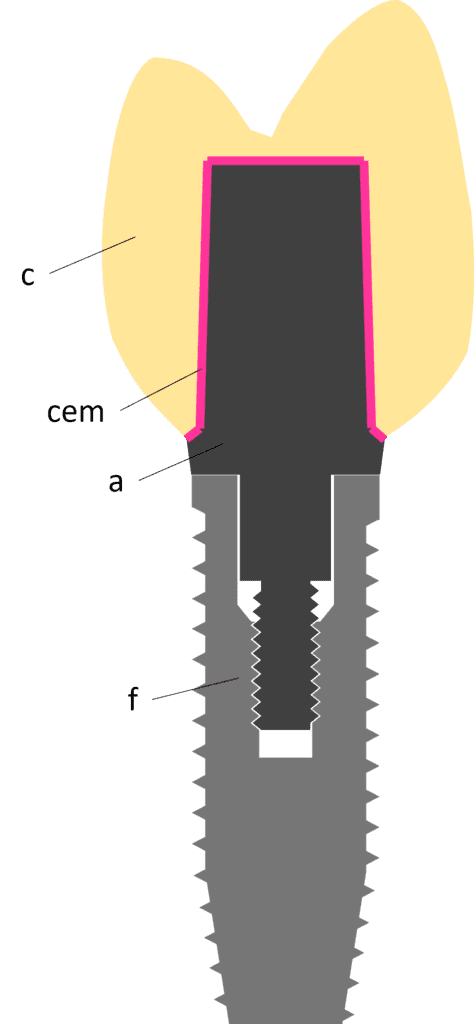
Figure 2
Implant abutments act as the connector between the fixture and the prosthesis. It is important to understand that all abutments, regardless of their intended connection to the prosthesis are always screwed down to the fixture through a screw channel, whether it be with a separate screw or, very infrequently, as a one piece abutment where the screw is “built in” to the abutment (Figure 2). Therefore, even prostheses that are cemented and have the intention of covering the screw channel, will still have an abutment with a screw fixation mechanism to the fixture. The presence of this abutment screw does not determine what is referred to as cement-retained or screw-retained.
To make definitions even more vague, prostheses can be cemented to the abutment not by the clinician in the patient’s mouth, but rather done so in the laboratory before being connected to the fixture. In these cases, there is a “hole” or channel cut into the prosthesis so that the pre-cemented prosthesis and abutment can be screwed down to the fixture in one piece. These are known as direct-to-fixture prostheses, and despite still using cement to fixate the prosthesis to the abutment, they are not considered “cement retained” by the literature.
Definition and Examples of Cement-Retained Implant Supported Prostheses
The few articles that do provide some degree of clarification of definitions essentially infer that cement retention is any implant restoration that is not only fixated to the abutment using dental cements, but also covers the screw channel in order to achieve better occlusion and better aesthetics. The improved occlusion is due to the fact that load can be applied directly through the axis of the fixture. This is because the prosthesis covers the screw channel, and the screw channel will always be in line with the axis of the fixture. If this screw channel is not covered by the prosthesis, occlusal forces cannot be applied to the prosthesis through the axis, and this creates a cantilevering force which is considered to be destructive to the fixture, abutment and prosthesis complex.11 The improved aesthetics is a result of the absence of a visible screw channel, which even if covered in opaque composite, rarely matches the colour of the prosthesis exactly.12 In these cement-retained prosthesis situations, it is important to understand that the abutment is still invariably screwed down to the fixture.
Given the description above, cement-retained implant prostheses should be defined in the literature as prostheses that are cemented clinically in the patient’s mouth, after which there is no other means of accessing the prosthetic or abutment screw without cutting the crown. Examples of cement-retained restorations as defined above, and inferred by the literature, will be described below with illustrations.
Figure 1 shows a stock (or pre-fabricated) titanium abutment (a) which is screwed via an abutment screw (as) to the fixture (f). There is a full zirconia crown (c) covering the screw channel cemented with a layer of cement (cem) to the abutment.
Figure 2 shows a stock one piece titanium abutment which has conjoined screw (a). The abutment itself is screwed into the fixture (f) with a full zirconia crown (c) cemented with a layer of cement (cem) to the abutment. There is no screw channel to cover since the abutment is a one piece abutment.
<< Back to Contents Menu
EDITOR’S PAGE | MESSAGE FROM THE CHAIR | NEWS | PRODUCTS | FEATURE ARTICLES | CLINICAL | Q&A | EXHIBITIONS & CONFERENCES | SLEEP APNOEA
Figure 3 shows a customised titanium abutment (a) which is screwed via an abutment screw (as) to the fixture (f). There is a full zirconia crown (c) covering the screw channel cemented with a layer of cement (cem) to the abutment.
Definition and Examples of Screw-Retained Implant Supported Prostheses
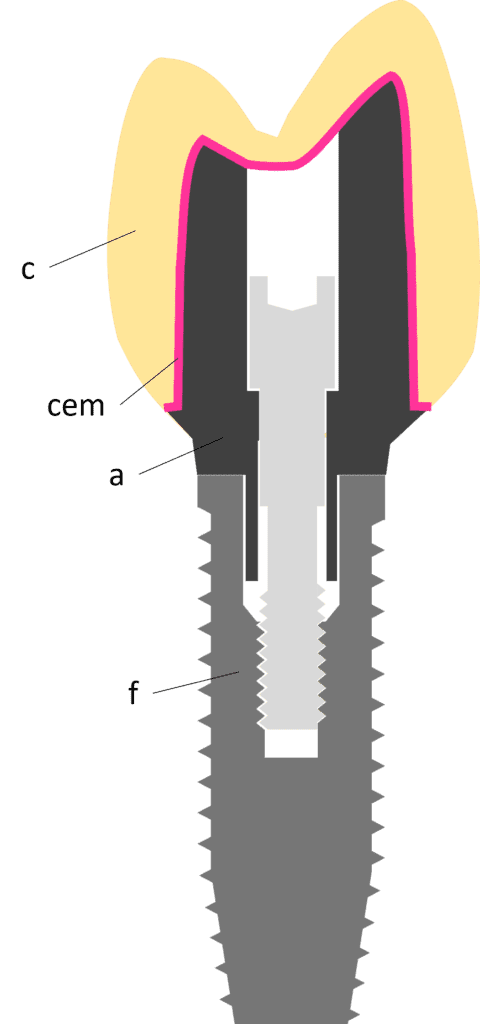
Figure 3
Figure 4
The literature infers that screw retention is any prosthesis “attachment mechanism that sacrifices occlusion and esthetics for retrievability”. This means that there is a screw channel present through the prosthesis, for the purposes of access to an internal screw. This internal screw may be an abutment screw, in the case of a direct-to-fixture prosthesis; or a prosthetic screw, in the case of a prosthesis that connected to the abutment via a second screw. The screw channel needs to be filled with a restorative material, and the occlusal contacts on the prosthesis must then be shifted away from this channel, meaning all occlusal forces become non-axial relative to the implant. These non-axial or cantilevering forces are considered to be destructive, and can result in screw loosening or fracture, and increased micro leakage.11 The loss of integrity due to the screw channel also increases risk of prosthetic fracture.7 It is interesting to note that cross-pin restorations do not have a screw channel, and do not sacrifice occlusion or aesthetics, but are still considered to be screw retained restorations.
Given the description above, screw-retained implant prostheses should be defined as prostheses where there is direct access to the prosthetic or abutment screw when inserted into the patient’s mouth. The screw channel, if present, may then be covered in any other restorative material. Examples of screw-retained restorations as defined above, and inferred by the literature, will be described below with illustrations.
Figure 4 shows a customised base metal abutment (a) which is screwed via an abutment screw (as) to the fixture (f). There is a feldspathic ceramic layer (c) fired directly to the surface of the abutment, obviating the need for cement. There is a screw channel present to gain access to the abutment screw. Since the prosthesis and abutment are already joined before insertion to the fixture, this is also known as a direct-to-fixture restoration.
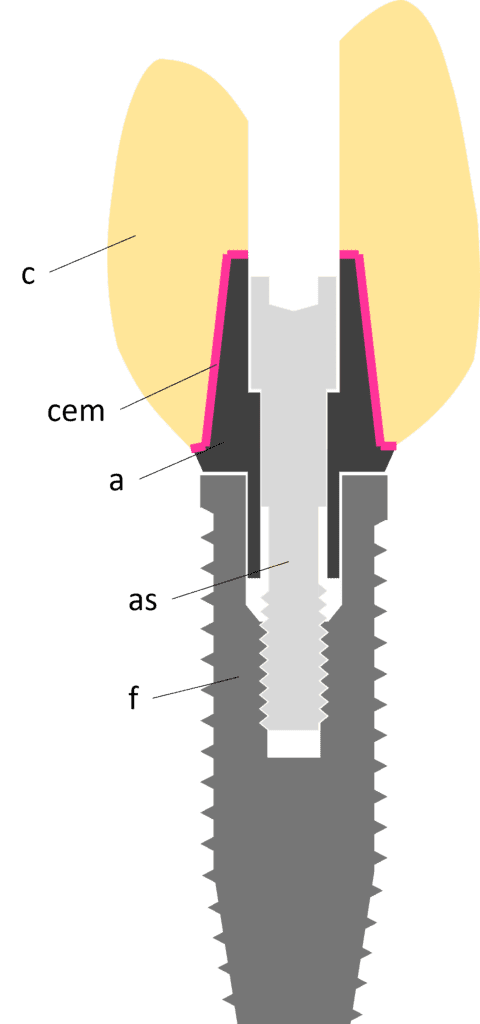
Figure 5 shows a stock titanium abutment (a) often referred to as a “Ti-base” which is screwed via an abutment screw (as) to the fixture (f). There is a full zirconia crown (c) pre-cemented with a layer of cement (cem) to the abutment, but there is a hole present to gain access to the screw channel. Despite the use of cement, this is still regarded as a screw-retained prosthesis. This is also a direct-to-fixture restoration.
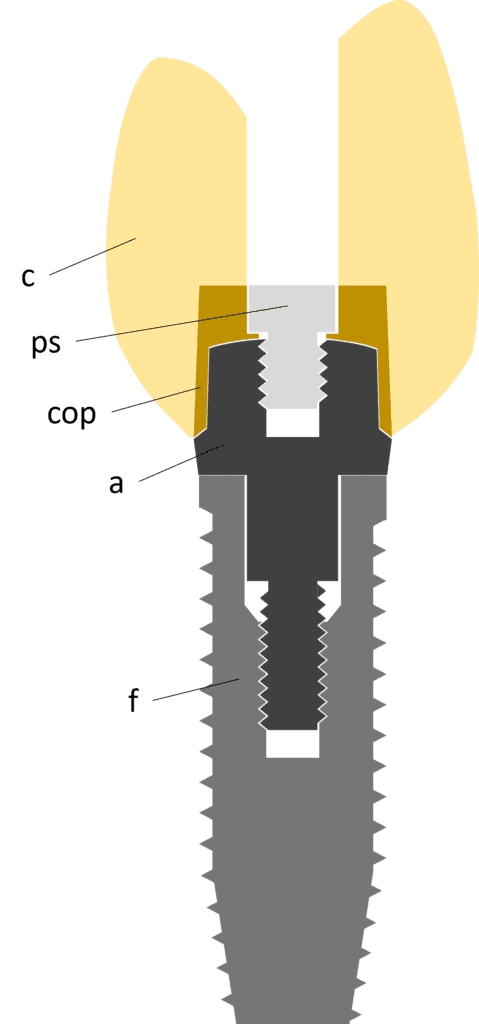
Figure 6 shows a stock one piece titanium abutment (a) which has a conjoined screw. The abutment itself is screwed to the fixture (f). There is a porcelain-fused-to-metal crown (c) cast onto a metal coping (cop), and there is a screw channel present in the crown to gain access to a 2nd screw, the prosthetic screw (ps), that holds the crown and coping to the abutment.
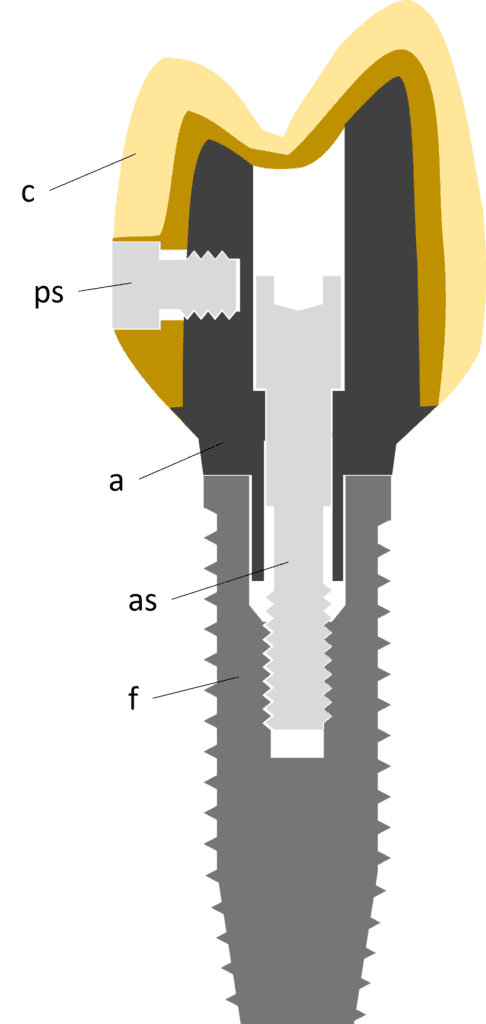
Figure 7 shows a customised titanium abutment (a) which is screwed via an abutment screw (as) to the fixture (f). There is a porcelain-fused-to-metal crown (c) that is screwed to the abutment from the palatal surface using a cross-pin prosthetic screw (ps). The crown covers the screw access channel allowing occlusal forces to be directed through the axis of the fixture and improves aesthetics, but this is not regarded as a cement-retained prosthesis.
Clinical Identification and Retrieval of Cement-Retained vs Screw-Retained Prostheses
From a clinical standpoint, cement-retained implant prostheses can be distinguished by the absence of either a screw access channel covered in restorative material, or the absence of a cross pin screw. If the internal abutment screw becomes loosened or disengages completely from the fixture, retrieval techniques include attempted removal of crown (crown removers or completely cutting the crown off) or by cutting a hole through the crown, essentially converting it into a direct-to-fixture restoration.
Screw-retained restorations can be clinically identified by the presence of a screw-access channel or a cross-pin screw. Retrieval or re-tightening a loose screw is much simpler and involves removal of the restorative material covering the internal screw; or in the case of a cross-pin, direct access to the cross-pin screw is immediately obtainable from the palatal/lingual surface.
Conclusions
Cement-retained implant prostheses should be defined in the literature as prostheses that are cemented clinically in the patient’s mouth, after which there is no other means of accessing the prosthetic or abutment screw without cutting the crown.
Screw-retained implant prostheses should be defined as prostheses where there is direct access to the prosthetic or abutment screw when inserted into the patient’s mouth. The screw channel, if present, may then be covered in any other restorative material.
- Hebel KS, Gajjar RC. Cement-retained versus screw-retained implant restorations: achieving optimal occlusion and esthetics in implant dentistry. The Journal of prosthetic dentistry. 1997 Jan 1;77(1):28-35.
- Lv XL, Qian SJ, Qiao SC, Gu YX, Lai HC, Shi JY. Clinical, radiographic, and immunological evaluation of angulated screw‐retained and cemented single‐implant crowns in the esthetic region: A 1‐year randomized controlled clinical trial. Clinical Implant Dentistry and Related Research. 2021 Oct;23(5):692-702.
- Al‐Omari WM, Shadid R, Abu‐Naba’a L, Masoud BE. Porcelain fracture resistance of screw‐retained, cement‐retained, and screw‐cement‐retained implant‐supported metal ceramic posterior crowns. Journal of Prosthodontics: Implant, Esthetic and Reconstructive Dentistry. 2010 Jun;19(4):263-73.
- Michalakis KX, Hirayama H, Garefis PD. Cement-retained versus screw-retained implant restorations: a critical review. International journal of oral & maxillofacial implants. 2003 Sep 1;18(5).
- Wittneben JG, Joda T, Weber HP, Brägger U. Screw retained vs. cement retained implant‐supported fixed dental prosthesis. Periodontology 2000. 2017 Feb;73(1):141-51.
- Lemos CA, de Souza Batista VE, de Faria Almeida DA, Júnior JF, Verri FR, Pellizzer EP. Evaluation of cement-retained versus screw-retained implant-supported restorations for marginal bone loss: A systematic review and meta-analysis. The Journal of prosthetic dentistry. 2016 Apr 1;115(4):419-27.
- Torrado E, Ercoli C, Al Mardini M, Graser GN, Tallents RH, Cordaro L. A comparison of the porcelain fracture resistance of screw-retained and cement-retained implant-supported metal-ceramic crowns. The Journal of prosthetic dentistry. 2004 Jun 1;91(6):532-7.?
- Kim WD, Jacobson Z, Nathanson D. In vitro stress analyses of dental implants supporting screw-retained and cement-retained prostheses. Implant dentistry. 1999 Jan 1;8(2):141-51.?
- Crespi R, Capparè P, Gastaldi G, Gherlone EF. Immediate occlusal loading of full-arch rehabilitations: screw-retained versus cement-retained prosthesis. An 8-year clinical evaluation. International Journal of Oral & Maxillofacial Implants. 2014 Dec 1;29(6).?
- Wittneben JG, Millen C, Brägger U. Clinical Performance of Screw-Versus Cement-Retained Fixed Implant-Supported Reconstructions-A Systematic Review. International journal of oral & maxillofacial implants. 2014 Jan 2;29.?
- Kourtis S, Damanaki M, Kaitatzidou S, Kaitatzidou A, Roussou V. Loosening of the fixing screw in single implant crowns: predisposing factors, prevention and treatment options. Journal of Esthetic and Restorative Dentistry. 2017 Jul 8;29(4):233-46.
- Wadhwani C, Piñeyro A, Avots J. An esthetic solution to the screw‐retained implant restoration: introduction to the implant crown adhesive plug: clinical report. Journal of Esthetic and Restorative Dentistry. 2011 Jun;23(3):138-43.
The information and viewpoints presented in the above news piece or article do not necessarily reflect the official stance or policy of Dental Resource Asia or the DRA Journal. While we strive to ensure the accuracy of our content, Dental Resource Asia (DRA) or DRA Journal cannot guarantee the constant correctness, comprehensiveness, or timeliness of all the information contained within this website or journal.
Please be aware that all product details, product specifications, and data on this website or journal may be modified without prior notice in order to enhance reliability, functionality, design, or for other reasons.
The content contributed by our bloggers or authors represents their personal opinions and is not intended to defame or discredit any religion, ethnic group, club, organisation, company, individual, or any entity or individual.