


Abstract
Management of enamel hypoplasia induced by traumatic dental injuries (TDI) can pose a challenge for clinicians. Sequela of permanent tooth TDI during odontogenesis can lead to development disturbances ranging from minor to severe. Enamel hypoplasia is a quantitative defect in which plaque retentive enamel pitting increases caries risk, in addition to the unaesthetic discoloration. Treatment options of minor permanent tooth TDI developmental defects include bleaching, direct composite restoration (megabrasion), direct composite veneers and indirect restorations. This case report focuses on the treatment of enamel hypoplasia in a young adult utilising direct composite veneers.
Learning Objectives
This case report discusses the management of enamel hypoplasia as a consequence of TDI. The intended learning objectives include:
- Identify the different presentations of permanent tooth disturbances
- Understand treatment modalities for the management of minor disturbances induced by TDI to developing permanent teeth
- Introduction to the Paladex and Uveneer systems in the composite restorative workflow
Introduction
Traumatic dental injuries (TDI) involve damage to the dentition, periodontium and orofacial structures. Most TDI have been reported in the younger age groups which coincides with the development of the permanent dentition.1 Primary tooth TDI can either, directly damage the permanent tooth germ or, indirectly via a drop in pH from primary tooth pulpal necrosis (intracanal infection) with diffuse apical periodontitis; called Turner’s tooth.2
The main injuries that can alter development of permanent dentition include intrusive luxation and avulsion of the primary dentition. For intrusive primary tooth injuries, the clinician should allow spontaneous re-eruption regardless of the intrusion direction; typically, spontaneous re-eruption is seen within 6-12 months. Any avulsed primary tooth must not be replanted due to risk of trauma to the permanent germ. Radiographic assessment aids confirm suspected avulsion cases. For more comprehensive management of TDI follow the International Association of Dental Traumatology (IADT) 2020 guidelines.3

Follow-up is critical for early diagnosis of complications and management of healing. A subsequent radiograph is indicated prior eruption of permanent successors, to identify disturbances in tooth development and eruption.4
The type of permanent tooth damage sustained (Table 1) is dependent on the dental development stage in which the disturbance occurred, as well as the force and type of injury.4 Of these, minor disturbances such as enamel discolouration with or without hypoplasia are the most common sequelae.4
Hypoplasia is a quantitative enamel defect visible with tooth eruption unlike hypomineralisation; a qualitative defect with post-eruptive breakdown. Hypoplasia presentations vary in severity and increases caries risk as the pitted enamel harbours dental plaque. This case report focuses on composite resin management of enamel hypoplasia in order to restore an individual’s confidence to smile and ultimately increase their self-esteem.







Figures 6a-6c: Paladex right central palatal surface build-up with flowable composite matching enamel shade.
Figures 7a-7c: Uveneer right central labial build-up with packable composite.
Case Report
An eighteen-year-old male presented concerned with the “look of [his] front teeth”. Medical history recorded no significant findings. Trauma history revealed the patient fell at the age of two while playing. All maxillary deciduous incisors were avulsed. The permanent incisors experienced delayed eruption in addition to well-demarcated areas of yellow-brown enamel opacities with hypoplasia (Table 1(b)). The patient has an edge-to-edge incisor relationship and low confidence to smile with teeth.
Treatment:
- Preoperative photographs (Fig 1).
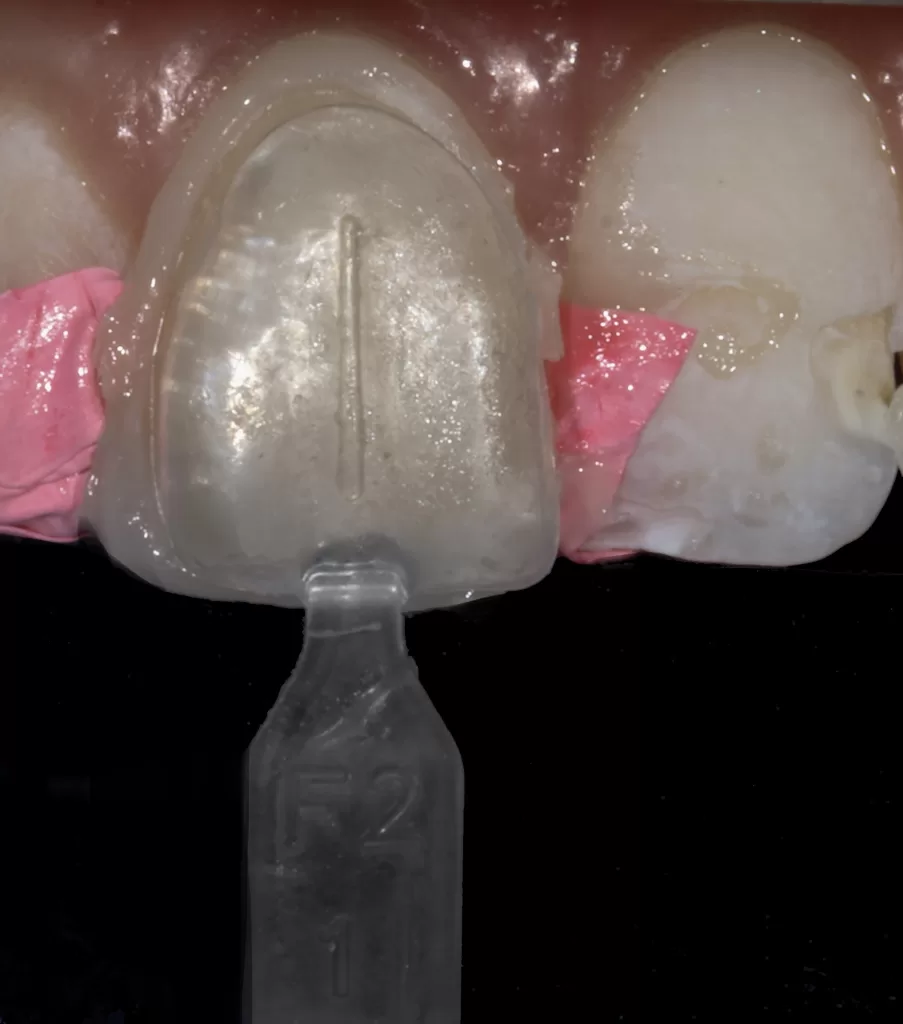
- Mock-up of final veneer to assess shade selection and ability to mask discolouration using Uveneer (Ultradent, South Jordan, Utah, United States) template (Fig 2).
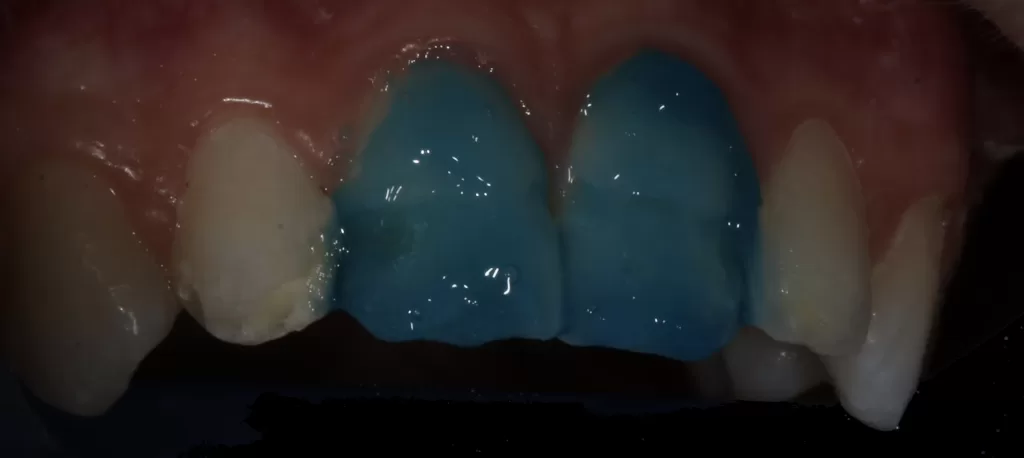
- Tooth isolation was ensured with the split dam technique placing a w2a clamp on the first maxillary premolars. This allows optimal moisture control while at the same time the ability to visualise maxillary anterior teeth alignment during the restorative build-up.
- Enamel surface freshened with coarse diamond bur.
- Enamel and dentine sandblasted with Aquacare Twin Aluminium Oxide 29 micron, rinsed and dried (Fig 3).
- Phosphoric acid etch for 15 seconds, washed and dried to frosted appearance (Figs 4a & 4b).
- Scotchbond Universal Adhesive (3M, St. Paul, Minneapolis, United States), rubbed 20 seconds, gentle air dry to dissolve the solvent, light cured 10 seconds (Fig 5).
- Palatal build-up utilising Paladex silicone matrix and enamel shade flowable high filled composite (Figs 6a-6c).
- IPS Empress Direct Bleach-L (Ivoclar, Schaan, Liechtenstein) was applied on the tooth as the bulk first layer composite and cured.
- IPS Empress Direct Bleach-L (Ivoclar, Schaan, Liechtenstein) was reapplied for second layer to optimise the masking characteristics of the composite and left uncured.
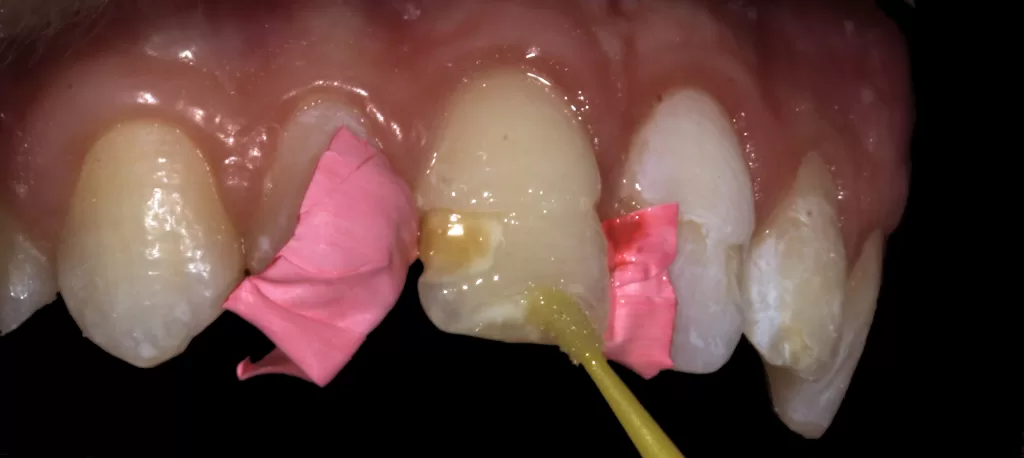
- While uncured Uveneer Extra template with G-aenial Injectable Bleach White (GC, Bunkyo-ku, Tokyo, Japan) is pressed as the final layer (aligning the vertical groove on the Uveneer with the long axis of the tooth) and light cured (Figs 7a-7c). Repeat steps 6-11 for the adjacent veneered teeth (Fig 8a).
- The purpose of two Ivoclar composite layers is to increase the opaqueness and mask the underlying tooth shade (Fig 8b). In contrast, the purpose of the injectable high filled composite is to capture the facial anatomy of the Uveneer and establish a natural long-lasting gloss. (Fig 8c).
- Final polishing: completed with sof-lex (3M, St. Paul, Minneapolis, United States) followed by diamond polishing paste (Ultradent, South Jordan, Utah, United States) on the FlexiBuff disc (Cosmedent, Chicago, Illinois, United States).
- The patient is then seated upright to determine the final incisal level balancing with the resting lip contours and interpupillary line (Figs 9a-9c).
- Evaluate postoperative outcome and occlusion (Figs 10a-10b, 11).
- Balanced incisal edge contacts during edge-edge static relationship to avoid stress in one area of the composite veneers





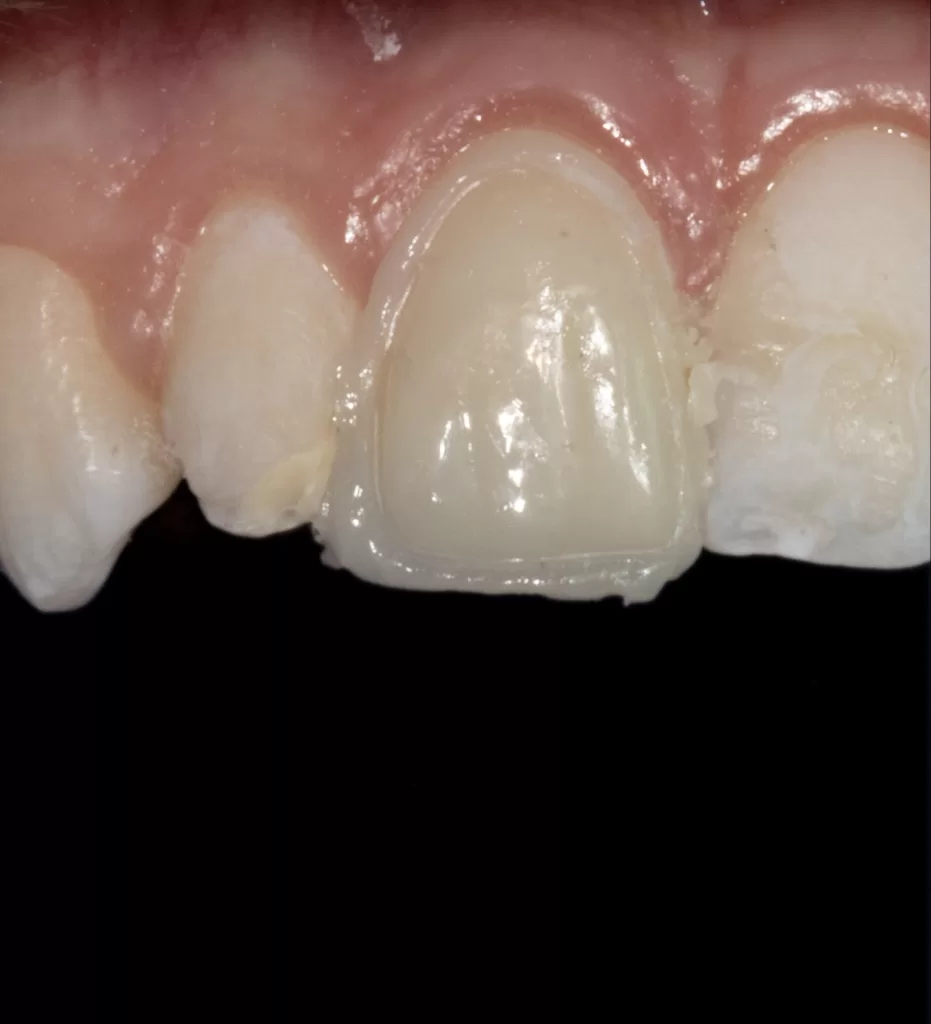
Figures 9a & 9b: Finish and polish.




Figure 11: Postoperative photograph.
Discussion
Diagnosis of TDI requires thorough history collection, clinical examination, and special testing. One should not automatically exclude alternative causes to enamel defects such fluorosis, childhood infections, hypoparathyroidism and metabolic disturbances (including rickets and celiac disease).4
Avulsion of primary teeth has been reported to affect up to 74.1% of the permanent successors.5 This occurs due to the proximity of the deciduous apex with the developing tooth germ. During avulsion the primary tooth root’s curvature produces a rotational movement that may injure the succedent bud. Depending on the timing of trauma a different stage of amelogenesis is disrupted. Amelogenesis is composed of three overarching stages:6

- Presecretory: Ameloblast prepare for the organic matrix synthesis. Defect here leads to enamel hypoplasia.
- Secretory: Highly organised enamel is laid down. Defect here leads to enamel hypoplasia.
- Maturation: Mineralisation of enamel. Defect here leads to enamel hypomineralisation.
Permanent incisor crowns complete development at age three. Any injury before this time damages ameloblasts leading to enamel defects (Table 1(b & c)).
Given TDI usually occurs at 0-2 years and coincides with the incisor crown formation, enamel defects (such as hypoplasia) are one of the most prevalent sequelae.7 TDI after radiographically visible complete crown formation (i.e. after the age of three for incisors) can lead to root dilaceration (Table 1E) and enamel discolouration (Table 1(a)); as maturation continues until eruption.8 If trauma corresponds to the maturation phase, ruffle-ended ameloblasts are damaged. Subsequent ameloblast metaplasia to cuboidal or squamous epithelium occurs leading to a reduction in inorganic content.2
As a result, a lower mineral content is incorporated into the enamel. Areas of reduced mineralisation have a differing refractive index (1.33 when filled with water compared to 1.62 of sound enamel) and thus clinically appear white.9 If trauma induced bleeding of the surrounding soft tissue occurs (even after cessation of ameloblast activity), the breakdown of haemoglobin will lead to the yellow-brown discolourations incorporating into the enamel.10
<< Back to Contents Menu
EDITOR’S PAGE | MESSAGE FROM THE CHAIR | NEWS | PRODUCTS | FEATURE ARTICLES | CLINICAL | Q&A | EXHIBITIONS & CONFERENCES | SLEEP APNOEA

Management of minor yellow-to-white opacities may be aesthetically managed with micro-abrasion.8 A by-product of micro-abrasion is the increase in light absorption and thus further reduction in refractive index compared to sound enamel leading to reduced value and increase in chroma shining through the enamel.11
As such, combination of micro-abrasion and extrinsic bleaching may aid break the double bonds of chromophores that give the tooth some of its chroma. Regardless, often TDI caused discolorations span the entire enamel thickness, as such, micro-abrasion and bleaching combination can lead to the negative amplification of the opaque discolouration. Megabrasion is more clinically reliable; utilising high-speed bur to remove the defective enamel followed by adhesive composite resin restoration.11
In this clinical report the patient desired aesthetic changes to the hypoplastic anteriors but declined orthodontic and orthognathic surgery for correction of the prognathic mandible. Restorative options were thus restricted to direct or indirect veneers.
Given adolescence is a crucial developmental phase in building confidence, the patient rejected indirect veneers as they contained too many barriers between him and restoring his self-esteem.
This included tooth preparation, need for full periodontal maturity, greater number of visits and higher fees.

As such, the patient elected for the direct restorative method, which can be conducted in one of three main ways (Table 2):
- Free hand
- Stent
- (a) Laboratory-made palatal putty stent.
- (b) Uveneer, with or without the Paladex system.
- (c) Injectable technique.
Advantages of composite veneers include the ability to be completed at any age post-eruption, unlike porcelain veneers which require the individual to reach full periodontal maturity. Further, the direct approach allows easy chairside maintenance and repairs.
Stents provide the operator with more predictability and clinical efficiency with the additional advantage to preventing formation of the oxygen inhibition layer. This is evident in both the Uveneer system and injectable technique, as the final composite layer is cured through an oxygen barrier that still facilitates light transmission.
Enamel’s semi-translucency is not easily simulated. A preoperative mock-up aids not only to select the correct hue, chroma and value but also match its opalescent likeness. Often clinicians disregard the thickness of the final restoration in the mock-up phase resulting in an intensified final chroma or opaqueness. To improve likeness of the mock-up to the final shade ensure a sufficient composite thickness is tested to assess its suitability.

In order to maximise adhesion a 29-micron aluminium oxide air abrasion (Velopex AquaCare Twin, Willesden, London, England), pre-treatment was utilised under split rubber dam technique to protect the patient’s airway. Aluminium oxide air abrasion prior to an etch-and-rinse system increases the longevity of the composite restorations by significantly improving bond strength (from 33.78MPa to 55.08MPa) (Fig 12).12 This is explained by an increase in surface area, surface free energy and wettability of dentine and enamel to the adhesive.11
Given the desire to mask the underlying hypoplastic discoloration the injectable technique was rejected as it does not readily allow separate layering of composite resin to achieve the desired masking properties. Additionally, the injectable technique burdens patients with an increase in laboratory cost for construction of injectable stent. Rather, the Uveneer and Paladex systems were selected as they increase predictability compared to free-hand composite build-up, allow incremental composite layering to increase hypoplastic masking property and are more cost-effective relative to a wax-up and laboratory-made palatal putty stent (Table 2).
The Paladex (Dental Art Innovations, City of Glen Eira, Victoria, Australia) (Figs 6a-6c & 13) is a silicone palatal index that adapts to the palatal surface replacing traditional silicone palatal keys.
For the bulk of the veneer, two increments of the same shade of composite are layered; curing each layer separately. The aim of this method is to create the opaqueness to mask the underlying hypoplastic tooth shade (Figs 8b & 8c).
Once the palatal aspect has been established using the Paladex, the facial is built using a first layer of packable composite that is light cured followed by a second packable composite layer pressed with the Uveneer and left uncured. The Uveneer is then lined with high filler flowable composite (Figs 7a-7c, 8a-8c & 14), pressed onto the uncured second layer of packable composite and cured together; reproducing the aesthetically natural facial anatomy based on Dr. Jan Hajtó’s natural ‘Anteriores’.13
Collectively, these tools were utilised over the free-hand technique, to save time and improve predictability, and over the injectable technique to allow separate layer application to mask the hypoplastic discolouration.
Conclusion
TDI most frequently occur in children during the development of permanent dentition. The ramifications to the succedent teeth ranges from discoloration’s and enamel hypoplasia to more severe dilaceration and root angulations. Restoring hypoplastic teeth not only provides a smoother less plaque retentive surface to promote oral hygiene but also re-establishes aesthetics and in doing so the confidence to smile.
References
- 1.Lam R. Epidemiology and outcomes of traumatic dental injuries: a review of the literature. Aust Dent J. 2016 Mar;61 Suppl 1:4-20.
- 2.Valderhaug J. Periapical inflammation in primary teeth and its effect on the permanent successors. Int J Oral Surg. 1974;3(4):171-82.
- 3.Day PF, Flores MT, O’Connell AC, Abbott PV, Tsilingaridis G, Fouad AF, Cohenca N, Lauridsen E, Bourguignon C, Hicks L, Andreasen JO, Cehreklui ZC, Harklamb S, Kahler B, Oginni A, Semper M, Levin L. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 3. Injuries in the primary dentition. Dent Traumatol. 2020 Aug;36(4):343-59.
- 4.Andreasen JO, Bakland LLK, Flores MT, Andreasen FM, Anderson L. Traumatic dental injuries : a manual. 3rd ed. Chichester, West Sussex: Chichester, West Sussex : Wiley-Blackwell; 2011. https://www.wiley.com/en-us/Traumatic+Dental+Injuries:+A+Manual,+3rd+Edition-p-9781405190619
- 5.Ravn JJ. Developmental disturbances in permanent teeth after exarticulation of their primary predecessors. Scand J Dent Res. 1975 May;83(3):131-4.
- 6.Nanci A. Ten Cate’s oral histology: development, structure, and function. 9th edition. St. Louis, Missouri : Elsevier; Dec 2018. https://www.elsevier.com/books/ten-cates-oral-histology/nanci/978-0-323-48518-0
- 7.Flores MT, Onetto JE. How does orofacial trauma in children affect the developing dentition? Long‐term treatment and associated complications. Dent Traumatol. 2019 Dec;35(6):312-23.
- 8.Andreasen JO, Andreasen FM (Frances M), Andersson L. Textbook and color atlas of traumatic injuries to the teeth. 5th edition. Hoboken, NJ : Wiley-Blackwell; Dec 2019. https://www.wiley.com/en-us/Textbook+and+Color+Atlas+of+Traumatic+Injuries+to+the+Teeth,+5th+Edition-p-9781119167051
- Kidd EAM, Fejerskov O. What constitutes dental caries? histopathology of carious enamel and dentin related to the action of cariogenic biofilms. J Dent Res. 2004;83 Spec No C:C35-8. doi: 10.1177/154405910408301s07.
- Andreasen JO, Sundström B, Ravn JJ. The effect of traumatic injuries to primary teeth on their permanent successors. I. A clinical and histologic study of 117 injured permanent teeth. Scand J Dent Res. 1971;79(4):219-83.
- Magne P, Belser U. Bonded porcelain restorations in the anterior dentition : a biomimetic approach. Hanover Park (IL): Quintessence Pub.; 2002. P. 179-204.
- Sutil BGDS, Susin AH. Dentin pretreatment and adhesive temperature as affecting factors on bond strength of a universal adhesive system. J Appl Oral Sci. 2017 Sep-Oct;25(5):533–40.
- Hajtó J. Anteriores: Picture gallery. Bd. 2. Teamwork Media; 2006.
The information and viewpoints presented in the above news piece or article do not necessarily reflect the official stance or policy of Dental Resource Asia or the DRA Journal. While we strive to ensure the accuracy of our content, Dental Resource Asia (DRA) or DRA Journal cannot guarantee the constant correctness, comprehensiveness, or timeliness of all the information contained within this website or journal.
Please be aware that all product details, product specifications, and data on this website or journal may be modified without prior notice in order to enhance reliability, functionality, design, or for other reasons.
The content contributed by our bloggers or authors represents their personal opinions and is not intended to defame or discredit any religion, ethnic group, club, organisation, company, individual, or any entity or individual.